Kayla Jonas, Cameron J. Skaggs, Elizabeth Catalano, Lexi Bray, Erik Barfuss, Dr. Julia Oxford
Background
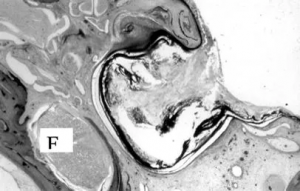
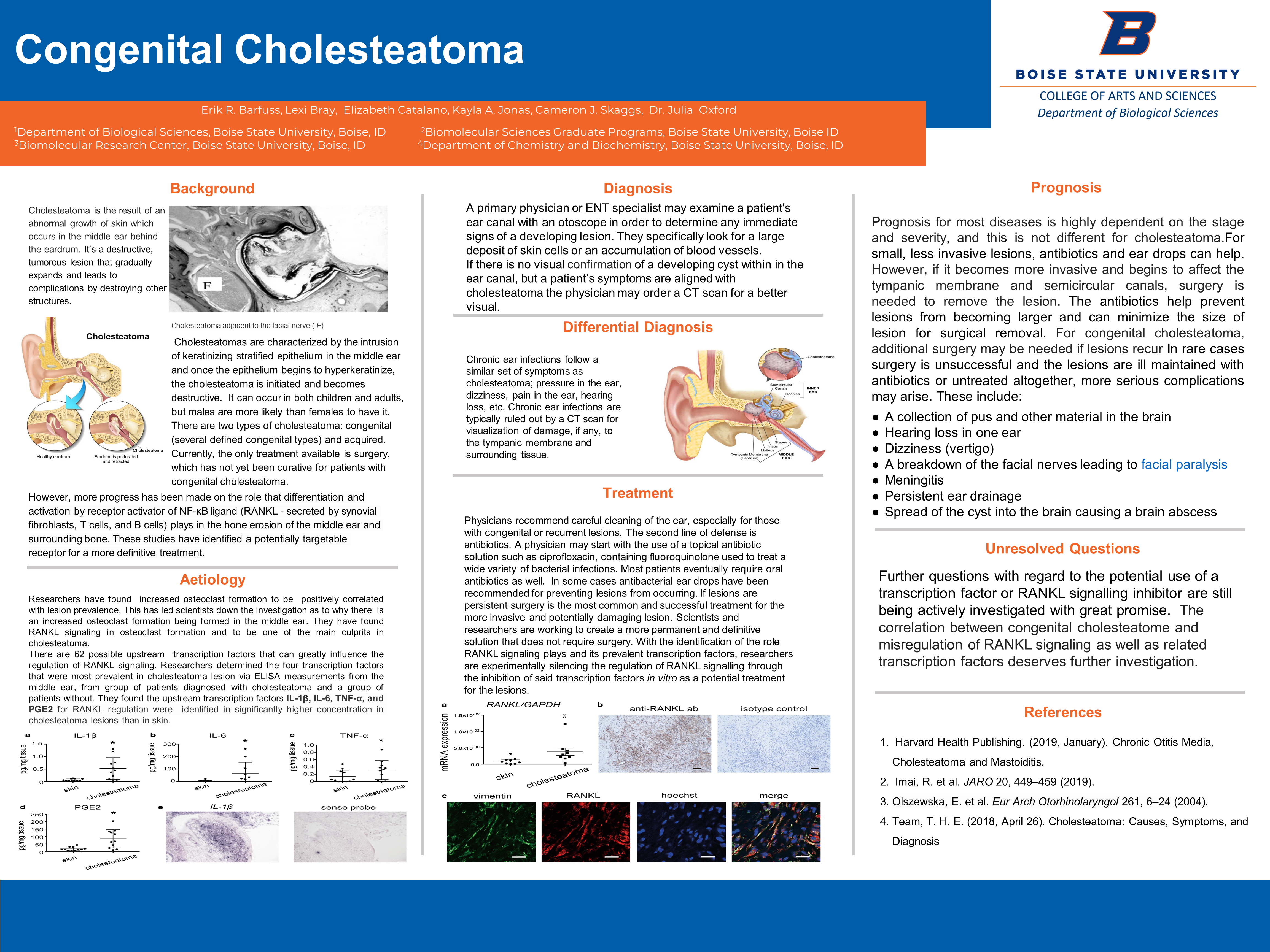
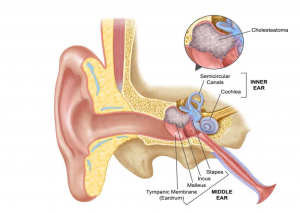
Cholesteatoma is the result of an abnormal growth of skin which occurs in the middle ear behind the eardrum. It’s a destructive, tumorous lesion that gradually expands and leads to complications by destroying other structures.
Cholesteatomas are characterized by the intrusion of keratinizing stratified epithelium in the middle ear and once the epithelium begins to hyperkeratinize, the cholesteatoma is initiated and becomes destructive. It can occur in both children and adults, but males are more likely than females to have it. There are two types of cholesteatoma: congenital (several defined congenital types) and acquired. Currently, the only treatment available is surgery, which has not yet been curative for patients with congenital cholesteatoma.
However, more progress has been made on the role that differentiation and activation by receptor activator of NF-κB ligand (RANKL – secreted by synovial fibroblasts, T cells, and B cells) plays in the bone erosion of the middle ear and surrounding bone. These studies have identified a potentially targetable receptor for a more definitive treatment.
Aetiology
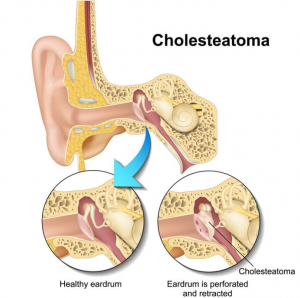
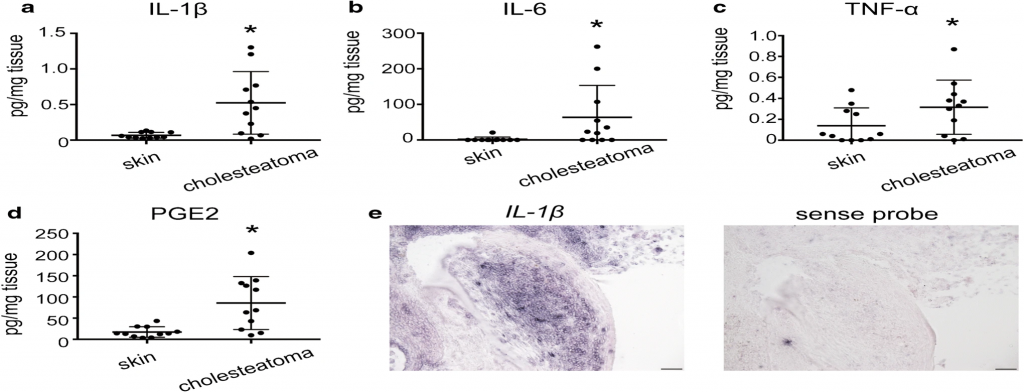
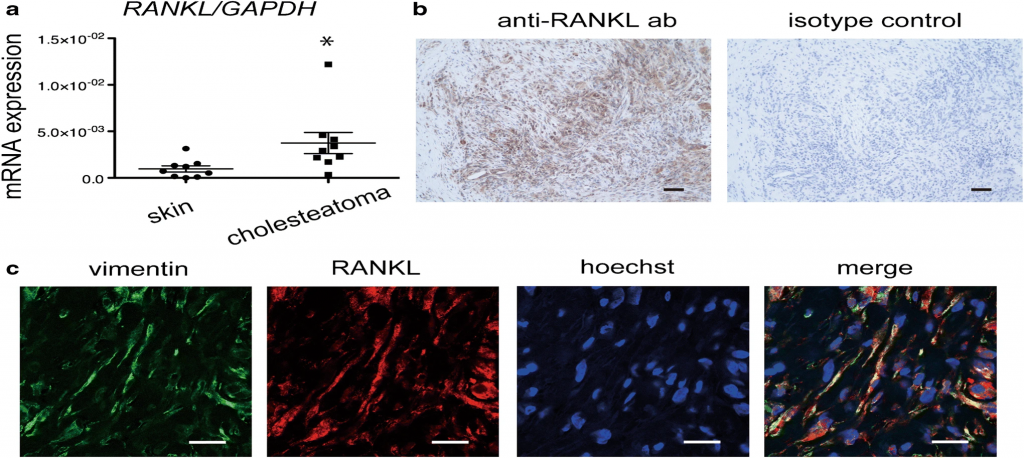
Researchers have found increased osteoclast formation to be positively correlated with lesion prevalence. This has led scientists down the investigation as to why there is an increased osteoclast formation being formed in the middle ear. They have found RANKL signaling in osteoclast formation and to be one of the main culprits in cholesteatoma.
There are 62 possible upstream transcription factors that can greatly influence the regulation of RANKL signaling. Researchers determined the four transcription factors that were most prevalent in cholesteatoma lesion via ELISA measurements from the middle ear, from group of patients diagnosed with cholesteatoma and a group of patients without. They found the upstream transcription factors IL-1β, IL-6, TNF-α, and PGE2 for RANKL regulation were identified in significantly higher concentration in cholesteatoma lesions than in skin.
Diagnosis
A primary physician or ENT specialist may examine a patient’s ear canal with an otoscope in order to determine any immediate signs of a developing lesion. They specifically look for a large deposit of skin cells or an accumulation of blood vessels.
If there is no visual confirmation of a developing cyst within in the ear canal, but a patient’s symptoms are aligned with cholesteatoma the physician may order a CT scan for a better visual.
Differential Diagnosis
Chronic ear infections follow a similar set of symptoms as cholesteatoma; pressure in the ear, dizziness, pain in the ear, hearing loss, etc. Chronic ear infections are typically ruled out by a CT scan for visualization of damage, if any, to the tympanic membrane and surrounding tissue.
Treatment
Physicians recommend careful cleaning of the ear, especially for those with congenital or recurrent lesions. The second line of defense is antibiotics. A physician may start with the use of a topical antibiotic solution such as ciprofloxacin, containing fluoroquinolone used to treat a wide variety of bacterial infections. Most patients eventually require oral antibiotics as well. In some cases antibacterial ear drops have been recommended for preventing lesions from occurring. If lesions are persistent surgery is the most common and successful treatment for the more invasive and potentially damaging lesion. Scientists and researchers are working to create a more permanent and definitive solution that does not require surgery. With the identification of the role RANKL signaling plays and its prevalent transcription factors, researchers are experimentally silencing the regulation of RANKL signalling through the inhibition of said transcription factors in vitro as a potential treatment for the lesions.
Prognosis
Prognosis for most diseases is highly dependent on the stage and severity, and this is not different for cholesteatoma.For small, less invasive lesions, antibiotics and ear drops can help. However, if it becomes more invasive and begins to affect the tympanic membrane and semicircular canals, surgery is needed to remove the lesion. The antibiotics help prevent lesions from becoming larger and can minimize the size of lesion for surgical removal. For congenital cholesteatoma, additional surgery may be needed if lesions recur In rare cases surgery is unsuccessful and the lesions are ill maintained with antibiotics or untreated altogether, more serious complications may arise. These include:
- A collection of pus and other material in the brain
- Hearing loss in one ear
- Dizziness (vertigo)
- A breakdown of the facial nerves leading to facial paralysis
- Meningitis
- Persistent ear drainage
- Spread of the cyst into the brain causing a brain abscess
Unresolved Questions
Further questions with regard to the potential use of a transcription factor or RANKL signalling inhibitor are still being actively investigated with great promise. The correlation between congenital cholesteatome and misregulation of RANKL signaling as well as related transcription factors deserves further investigation.
References
- Harvard Health Publishing. (2019, January). Chronic Otitis Media, Cholesteatoma and Mastoiditis.
- Imai, R. et al. JARO 20, 449–459 (2019).
- Olszewska, E. et al. Eur Arch Otorhinolaryngol 261, 6–24 (2004).
- Team, T. H. E. (2018, April 26). Cholesteatoma: Causes, Symptoms, and Diagnosis
Additional Information
For questions or comments about this research, contact Kayla Jonas at kaylajonas@u.boisestate.edu.