Simulated to Represent Normal, ARDS and COPD Lung Conditions
Kathleen A. Davis, Heather P. Peterson, Alex R. Sanders, Lonny Ashworth
Background
The purpose of this study was to evaluate the occurrence of AutoPEEP in Volume A/C when ventilating normal, ARDS and COPD lung conditions on multiple ventilators. Ventilators evaluated were the Servo-i, Drager V500, PB 980 and CareFusion Avea. An expiratory time equal to 3 to 5 time constants was used in an attempt to prevent AutoPEEP.
Method
This study was completed using an IngMar Medical ASL 5000 electronic lung simulator (ASL 5000) configured to simulate normal, ARDS and COPD conditions. Parameters used: Normal lung: Cst 54 ml/cm H2O, Inspiratory Resistance (Rin) 13 cm H2O/L/sec, Expiratory Resistance (Rout) 12 cm H2O/L/sec; ARDS: Cst 39 ml/cm H2O, Rin 12 cm H2O/L/sec, Rout 14 cm H2O/L/sec; COPD: Cst 59 ml/cm H2O, Rin 22 cm H2O/L/sec, Rout 18 cm H2O/L/sec.1 All scenarios had a Pmus (patient effort) of 0 cm H2O. A 70 kg predicted PBW, with a tidal volume of 6 ml/kg, was used in Volume A/C. Settings were adjusted to achieve a minute ventilation of 90 ml/min/kg, 120 ml/min/kg and 150 ml/min/kg PBW. Respiratory rates used were 15, 20 and 25 BPM. PEEP was set at 5 cm H2O. Peak flow and I-time were adjusted to maintain an I:E ratio of 1:3 for normal and ARDS conditions, and an I:E ratio of 1:4 was used for COPD conditions. An EST was completed on each ventilator. The y-piece of the ventilator circuit was attached to the ASL 5000 using a 7023 Hans Rudolph 22 mm adapter, without an ETT. The same circuit was used for each ventilator. Data was automatically measured and stored on the ASL 5000.
Under normal, ARDS and COPD lung conditions, the Servo-i was configured to Vt/Ti with a decelerating flow waveform of 0% and a rate of 15 BPM used to achieve a minute ventilation of 90 ml/min/kg. Stabilization for one minute occurred before data were gathered for an additional two minutes. Data gathering was repeated under the same conditions with a rate of 20 BPM to achieve a 120 ml/min/kg minute ventilation, and 25 BPM to achieve a minute ventilation of 150 ml/min/kg. The same data gathering process was repeated with all four ventilators. A decelerating flow waveform was used on the PB980 and the CareFusion Avea for all conditions and respiratory rates. AutoFlow was turned on in all conditions and respiratory rates on the Drager V500.
Results
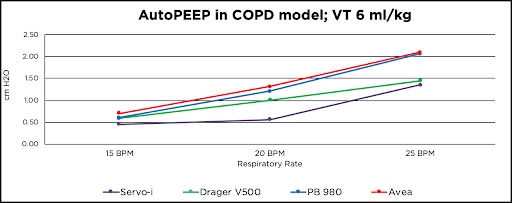
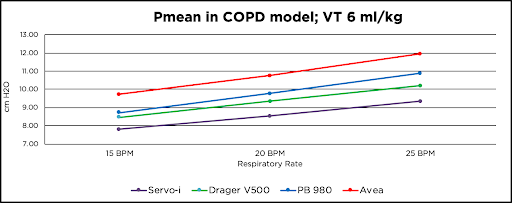
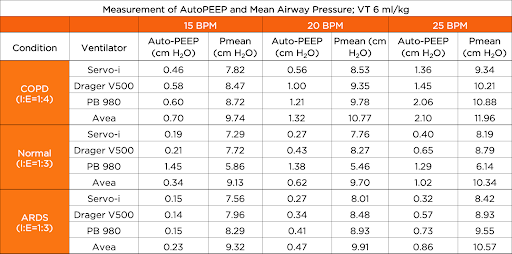
As respiratory rate increased, an increase in AutoPEEP was observed in each ventilator. The CareFusion Avea ended the COPD simulation with the highest amount of AutoPEEP at 2.10 cm H2O at 150 ml/min/kg and the Servo-i showed the lowest amount of AutoPEEP at 1.36 cm H2O at 150 ml/min/kg. Other findings showed that under normal conditions the PB 980 had the highest amount of AutoPEEP with all rate changes. Under COPD conditions the Servo-i had the overall lowest mean airway pressures; the CareFusion Avea showed the highest mean airway pressure at each lung condition and at each respiratory rate.
Conclusion
In Volume A/C, a reduction in expiratory time causes an increase in mean airway pressure, AutoPEEP, and Total PEEP in all conditions with all ventilators. The Servo-i showed the lowest amount of AutoPEEP, while the CareFusion Avea resulted in the highest AutoPEEP in COPD and ARDS conditions and the PB 980 had the highest AutoPEEP in normal conditions. Due to the possible physiological consequences of AutoPEEP and elevated mean airway pressures in critically ill patients, further research is needed to evaluate the presence of AutoPEEP and elevated mean airway pressures in the clinical setting with mechanically ventilated patients.
Limitation
The primary limitation of this bench study is that it was performed using an electronic lung simulator. Results of the study cannot be directly translated to patients. Additional clinical studies are necessary to evaluate the effect on AutoPEEP and mean airway pressure when using different ventilators.
References
- Arnal J., Garnero A, Saoli M & Chatburn RL (2018). Parameters for Simulation of Adult Subjects During Mechanical Ventilation. Respiratory Care, 63(2), 158–168. doi: 10.4187/respcare.05775
- No authors have a conflict of interest related to this research. No authors have received research funding, sponsorship or financial support from companies related to this research.
Additional Information
For questions or comments about this reasearch, contact Kathleen Davis at katiedavis1@u.boisestate.edu.